Healthcare App Development Company. We Build It. We Run It in Production.
Custom healthcare apps for post-discharge home recovery, 30-day readmission reduction, RPM, telemedicine, revenue cycle, and patient engagement. One of our production proof points: NeverAlone, the virtual care platform we built and operate, runs at 26K+ patients across 7 states.
Atlanta team, not a time zone away. The engineers in your discovery sessions write the code, ship it, and answer the phone when something breaks. PointClickCare and Gehrimed in production. Epic integrated in an R&D environment. FHIR, HL7, and ADT for the rest. 19 years of HIPAA-compliant builds.
Not every healthcare app should start as a full-scale platform. For new care models, pilots, or digital health concepts, we often recommend starting with a healthcare MVP to validate workflow, adoption, and ROI before scaling.





26K+
Patients in production across 7 states
96%
Treat-in-place rate, post-acute care
250K+
Calls handled across 130+ facilities
$20M+
Verified client ROI
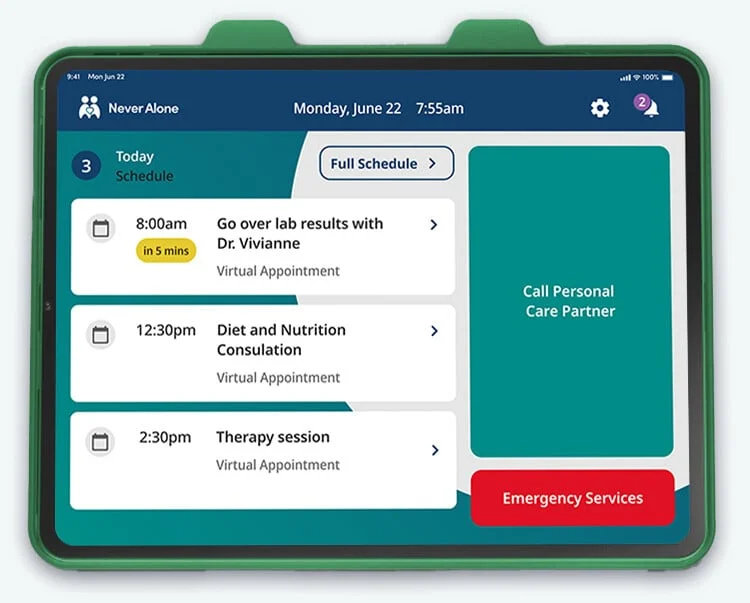
NeverAlone: A Healthcare App We Built, Run, and Expand Every Day
NeverAlone is a 24/7 virtual care platform that connects seniors, IDD individuals, and post-acute care residents with clinical care partners via real-time video. We didn’t hand this off, we built it, we operate it in production, and we continue to expand its capabilities across new care settings.
The platform integrates with pharmacy systems, EHRs, and third-party provider networks to deliver mission-critical care for CommuniCare Health Services, one of the largest post-acute providers in the country.
Calls Handled
Treat-in-Place
Facilities
States Live

Custom apps for post-discharge home recovery and 30-day readmission reduction.
High-risk elderly patients are most vulnerable in the first 30 days after discharge. A custom mobile app, paired with the right operating model, turns that window into measurable readmission avoidance, not a billing event.
NeverAlone is one of our production proof points for this use case. We built it. We operate it. 96% of clinical events get resolved in place, without sending the patient back to the hospital. That is a 30-day readmission story written in patient outcomes, not slides.
- Pulls discharge data from PointClickCare in production today. Epic integrated in an R&D environment. FHIR, HL7, and ADT for the rest.
- Connects high-risk elderly to a 24/7 clinical care partner via real-time video, before a hospital becomes the only answer.
- Surfaces chronic-condition risk signals from RPM devices, medication adherence, and patient-reported symptoms.
- Designed for the 85-year-old, not the 25-year-old engineer. Big targets, voice prompts, one-handed use, intermittent connectivity.
Named Use Cases We Build
Chronic-condition home recovery
CHF, COPD, post-surgical recovery, oncology home care. Daily check-ins, vitals, medication adherence, symptom escalation.
30-day readmission reduction
High-risk discharge cohorts get a 24/7 nurse line, RPM, and proactive outreach in the first 30 days. The window where readmission is preventable.
High-risk elderly support
Senior living, post-acute, IDD, home health, hospice. Bedside tablets and two-way video with a clinician trained for this population.
Treat-in-place virtual care
Resolve a clinical event without a hospital trip. NeverAlone runs at 96% treat-in-place across 130+ facilities.
Post-acute revenue cycle
RAF/HCC coding, MDS optimization, denial prediction. $10M PDPM revenue recovered on a single program.
You are the healthcare expert. We are your innovation partner.
Your team owns the clinical knowledge. We bring the engineering discipline to turn that knowledge into software your staff and patients actually use.
We are accustomed to working with doctors, nurses, care teams, patients, pharmacists, and the operations leaders who hold the workflow together. We know how to define new workflows when the right one does not exist yet, and how to integrate with existing ones when changing them is not the answer. The line between “new” and “existing” is where most healthcare software fails.
We do not pretend to be the clinician in the room. We pretend to be the partner who can ship the thing the clinician needs.
From clinical need to production app
One integrated team handles product strategy, UX research, engineering, and ongoing operations. The same people who observe your clinical workflows write the code that ships to production.
Discover
Understand the clinical problem, the users, the regulatory constraints. Define what to build, and what not to build.
Strategy + prioritized features
Phase 2Experiment
Prove the idea works before committing to a full build. Prototype, test with real clinicians, and validate the riskiest assumptions first.
Working prototype + clinical validation
Phase 3Engineer
Build production-quality healthcare software in iterative sprints. HIPAA-compliant infrastructure, EHR integrations, and the testing rigor clinical software demands.
Production app + launch
Phase 4Optimize
Scale based on real usage data. Expand to new care settings, add capabilities, and continuously improve. Healthcare apps are never “done”, they evolve with the care model.
Growth + continuous improvement
Healthcare apps running right now

NeverAlone
24/7 virtual care across 130+ facilities
Telehealth · Post-Acute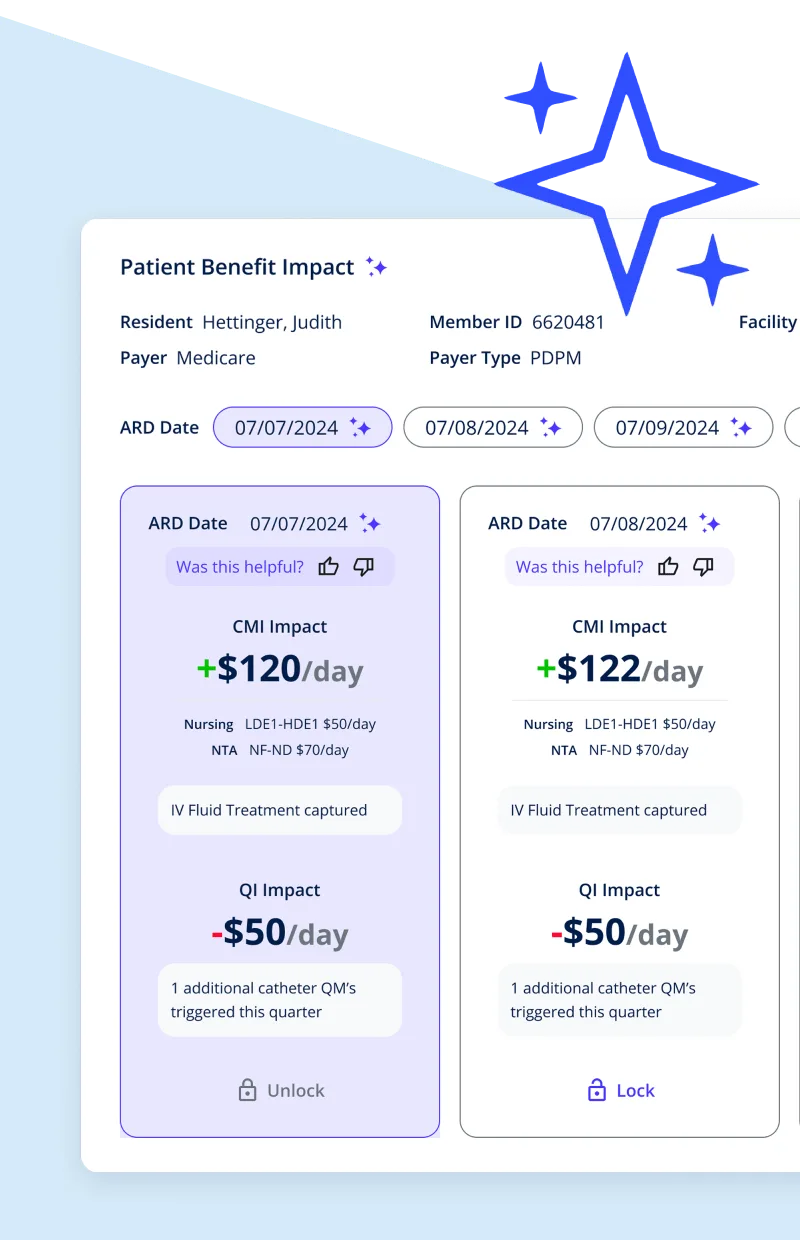
MDS Optimization
AI-driven coding recovers $10M+ in PDPM revenue
AI · Revenue Cycle
Guardian
AI-powered remote monitoring for the OR
AI · IoT · Mobile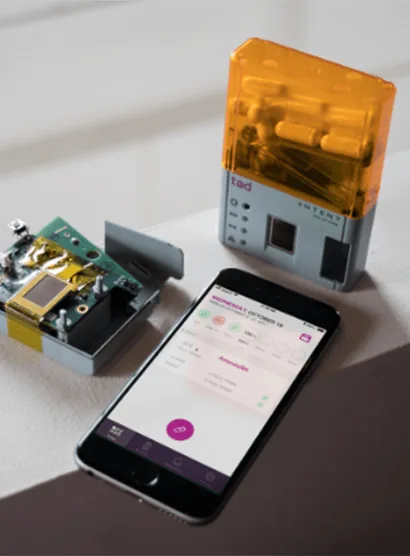
Intent Solutions
IoT smart pill bottle improves adherence
IoT · Bluetooth · MobileWe don't just write code. We run healthcare software in production.
Your phone is a sensor, your tablet is a care station, and your monitoring device is mission-critical. We build for all of them.
24/7 Production Operations
We operate NeverAlone around the clock, 130+ facilities, 7 states, 250K+ calls handled on the platform. When a fall alert fires at 2 AM, our infrastructure has to work. That operational discipline informs every product we build.
Hardware-Aware Development
Bedside tablets, OR monitors, Bluetooth pill bottles, wearable vitals sensors, healthcare doesn't live on a laptop. We design for intermittent connectivity, device provisioning at scale, and the physical reality of clinical environments.
HIPAA From Day One
PHI encryption, audit logging, role-based access mapped to clinical hierarchies, BAA-ready infrastructure. We don't bolt security on after the fact, it's in the architecture from sprint zero. We've passed audits. We know what surveyors look for.
What our healthcare clients say
“I have worked with many technology teams during my career, and Digital Scientists is one of the best. They take the time to understand the customers' needs, deliver innovative solutions, are always professional, and work with your team as a true partner to achieve success.”
AMY SEVERINO
chief innovation officer, NeverAlone (CommuniCare)
“By applying a robust machine learning model to our app, DS helped us create a scalable and accurate solution to improve the operating room experience for the anesthesia team and the patient. They are true collaborators.”
JUSTIN SCOTT, M.D., FASA
CEO, Vigilant Medical Solutions (Guardian)
“Digital Scientists provided immense value to our plan administrators, providers, and patients. The team was able to come in and understand our core needs, while remaining product agnostic. They helped identify the technical debt and pitfalls, and to get us to a point of stabilization and growth.”
ROBERT HAGER
CEO, CommuniCare Advantage
Where healthcare apps drive results
Remote Patient Monitoring
Continuous vital sign monitoring via connected devices. Proactive alerts reduce hospitalizations and enable treat-in-place care models.
RPM Solutions →Telehealth & Virtual Care
Video consultations, asynchronous messaging, and virtual rounding built for post-acute, home health, and primary care settings.
Telehealth Solutions →Clinical Decision Support
AI-powered tools that surface guidelines, flag risks, and recommend interventions at the point of care.
CDSS Solutions →Patient Portals & Digital Front Door
Self-service scheduling, health records access, secure messaging, and care plan tracking.
Digital Front Door →Revenue Cycle & Coding AI
Automated MDS coding, RAF/HCC score optimization, denial prediction, and claims workflow tools.
Revenue Cycle AI →EHR Integration & Interoperability
PointClickCare and Gehrimed in production. Epic integrated in an R&D environment. Bidirectional exchange with Cerner, MatrixCare, and other systems via HL7 FHIR, ADT feeds, and custom APIs.
Interoperability →Different ways to start a healthcare app project with us.
Pick the entry point that fits where you are, or schedule a free 30-minute consultation and we will help you choose.
Blueprint
$10K to $45K
1 to 4 weeks. Define what to build.
- • User research with clinicians and patients
- • Workflow design and architecture
- • Calibrated build proposal with milestones
- • Large tier ($45K) includes a functional prototype
Custom Build (Professional Services)
$250K to $1.5M
ROI in 12 to 36 months. Phased build.
- • You operate the care model. You own the IP.
- • Telehealth, RPM, EHR integration, payer billing
- • Milestone-funded, every phase a measurable outcome
- • HIPAA, BAA-ready, production launch
Equity-Aligned Build (Venture Studio)
Custom timeline
Equity or revenue-share, not fees.
- • Operator-founder partnerships and accelerator programs
- • When the model fits, we license a proven scaffold (e.g. NeverAlone for virtual care, 8 to 12 weeks)
- • Or co-build a custom platform with shared incentive
- • We have skin in the game
Other entry points: A one-day Working Session aligns the team on goals and constraints. A 5-day Validation Prototype ($20,000) ships HIPAA-compliant working software on your data when one technical assumption needs to be de-risked before a larger commit.
Not sure which is right? Talk to us first.
A free 30-minute consultation. No pitch. We will listen, ask questions about your workflow and constraints, and recommend the entry point that fits.
Schedule a free consultationHow to vet a healthcare app development partner.
If you are evaluating us against MindSea, Topflight, ScienceSoft, Arkenea, Vention, or Folio3, ask every firm the same eight questions. The right partner answers all of them in production terms, not slideware.
Have you operated a healthcare app you built in production?
Most firms ship and walk. The ones that operate the platform answer 2 AM pages know what production failure modes actually look like. DS operates NeverAlone 24/7 across 130+ facilities.
Name the EHRs you have integrated with by vendor.
Generic “FHIR / HL7 capability” is not the same as a production integration. Ask each firm to name vendors. DS has PointClickCare and Gehrimed in production and Epic integrated in an R&D environment, with FHIR, HL7, and ADT capability for the rest. No other firm in the comparison set publishes PointClickCare on its service page.
Show dollar-denominated outcomes from a single named program.
Project-level metrics are table stakes. Platform-level dollar outcomes are not. DS: $10M PDPM revenue recovered, $20M+ verified ROI, 96% treat-in-place across 26K+ patients.
Where is the team that writes the code? Same time zone as you?
Offshore staff augmentation is the cheap quote. It also produces the most rework. DS engineers are in Atlanta. The ones in your discovery sessions are the ones shipping the code.
Can you take equity instead of fees, if the model fits?
Pure services firms cannot. Equity-aligned partnership shifts the incentive from billable hours to outcomes. DS holds equity in NeverAlone and operates the platform we built. Our Venture Studio offers equity-aligned and operator-founder programs.
Show federal-compliance depth.
If you sell into VA, IHS, GSA, or any federal channel, your partner needs the compliance discipline that procurement expects. DS is in the GSA Multiple Award Schedule application process, the 13-month rigor that quality regulators apply to healthcare buyers as well.
Have you built for high-risk elderly / post-acute / home health populations?
Acute clinical-trial design is not the same as a tablet for an 85-year-old. DS lives in post-acute, SNF, senior living, home health, hospice, and IDD. CommuniCare, Easterseals, Guardian.
What do you charge to validate the riskiest assumption first?
A real partner will de-risk before billing six figures. DS Experiment: $20,000, 5 days, working software on your data. If the riskiest assumption fails, you saved $400K.
How we work together
Our engagements scale from a one-day session to a full product build. Pick the starting point that fits where you are.
Working Session
Align on goals, constraints, and next steps in a single day.
The Experiment
A working prototype in 5 days that proves whether the idea works.
Blueprint
Full architecture, scope, and a detailed plan before committing to the build.
Full Build
End-to-end healthcare app development, design through production launch.
Forward Deployed Engineering
AI agents deployed into healthcare workflows, integrated, governed, measurable.
Mobile isn’t a nice-to-have in healthcare. It’s the delivery mechanism.
Every day, nurses, CNAs, and clinicians depend on mobile apps to do their jobs. Patients use them to connect with their care team, manage chronic conditions, and access specialists they couldn’t reach otherwise. We build both sides of that equation, and we do it every day with NeverAlone for 26K+ patients across 7 states.
Workforce Utility at the Point of Care
Nurses and CNAs don’t have time to fight bad software. The apps they carry have to be fast, reliable, and designed for one-handed use during a shift. We build mobile tools that surface the right information at the right moment, medication schedules, vitals, care plans, so clinical staff spend time with patients, not screens. EHR interoperability (HL7 FHIR, ADT feeds, pharmacy systems) means these apps connect to the systems that already run the facility.
Patient Engagement & Rural Access
Mobile closes the gap between patients and their care teams. Video visits replace 90-minute drives. Medication reminders improve adherence. Secure messaging keeps patients engaged between appointments. For rural and underserved communities, a well-built mobile app isn’t convenience, it’s access. NeverAlone’s 96% treat-in-place rate proves what happens when the technology actually works for the patient, not just for the billing department.
Mission-Critical, User-Friendly
Healthcare apps must be both, reliable enough for a fall alert at 2 AM and intuitive enough for an 85-year-old using a tablet for the first time. That’s a UX research problem, not just a design problem. We run usability studies with real clinicians and real patients, test in actual care environments, and iterate based on observed behavior, not assumptions. The result is software people actually use, in settings where “I couldn’t figure it out” can mean a missed medication or a missed emergency.
Healthcare development thinking

What Is HIPAA and Why Does It Matter?
The compliance requirements every healthcare app developer needs to understand.
Read More →

How Clinical Decision Support Systems Drive Better Outcomes
CDSS tools that reduce diagnostic errors and improve evidence-based care.
Read More →

Healthcare UX Design: Why It Matters for Patient Outcomes
Why UX design is critical for EHRs, patient apps, and clinical workflows.
Read More →
Frequently Asked Questions
Common questions about healthcare app development, compliance, and working with Digital Scientists.
Start Here
See your healthcare app working in 5 days
Before committing to a full build, validate your concept with a functional prototype, HIPAA-compliant, on your data. $20,000. 5 days. Working software on your data.
Let’s Talk
30-minute conversation to understand your healthcare app challenge, identify opportunities, and see if there’s a fit. No pitch, just a conversation.
Or call: 404.654.3855