Technology Built for the Reality of Post-Acute Care
Multi-site operators face staffing shortages, reimbursement complexity, and after-hours coverage gaps across skilled nursing, home health, hospice, and senior living. We build production-proven technology that solves these problems at scale, not demos that never leave the conference room.




Post-acute care operators are fighting on three fronts simultaneously.
Post-acute care isn't a single setting, it's a continuum spanning skilled nursing, home health, hospice, assisted living, memory care, rehabilitation, and more. Each has different regulatory frameworks, payment models, and technology needs. The common thread: staffing shortages, reimbursement pressure, and technology that wasn't built for how these environments actually work.
One RN covering 100+ residents. When something goes wrong, the options are manage alone, call 911, or send to the ER. Each avoidable transfer costs $10K+ and triggers Medicare penalties.
Annual reimbursement leakage at a typical 100-facility operator from missed MDS diagnoses, undercoded assessments, and inconsistent PDPM capture across sites.
Per-visit documentation burden. Nurses spend more time charting than caring for residents. Documentation is the #1 driver of burnout, and burnout drives the staffing crisis.
Technology for Every Post-Acute Setting
We don't replace your EHR. We build technology that works alongside PointClickCare, MatrixCare, and Netsmart, filling the gaps that off-the-shelf platforms can't reach.
24/7 Virtual Care
Clinical coverage for nights, weekends, and after-hours across skilled nursing facilities. SBAR-based triage, EHR-integrated encounters, automated care coordination. 96% treat-in-place rate across 130+ facilities.
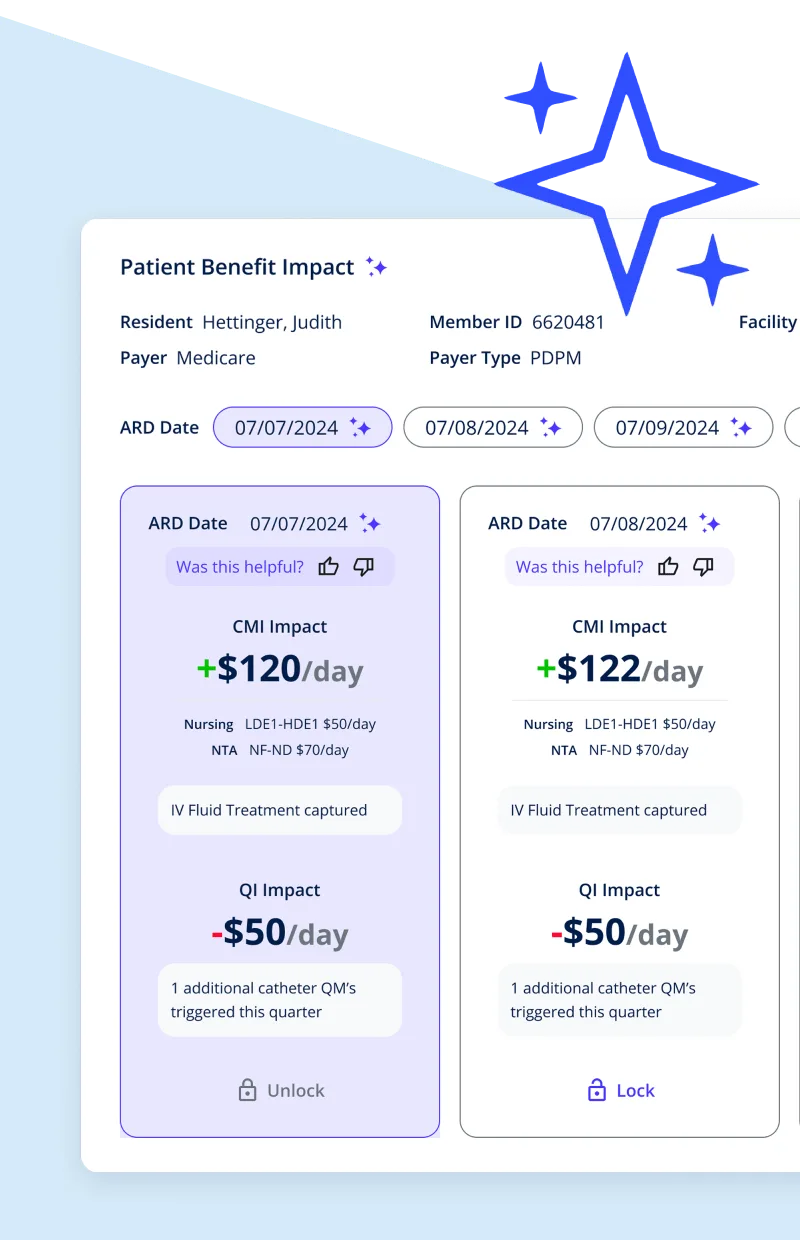
MDS/PDPM Optimization
AI-powered pre-submission audit that cross-references the full clinical record against the MDS. Catches diagnoses, comorbidities, and therapy minutes that manual reviews miss. $10M+ PDPM revenue recovered.
Ambient Documentation AI
Clinical documentation reduced from 45 minutes to 5 minutes per visit. Custom ambient scribes built for post-acute workflows, not repurposed from acute care.
RAF/HCC Coding AI
AI-assisted analysis of EHR and claims data to identify missed diagnosis codes for Medicare Advantage populations. $2.4M+ in compliant revenue recovery with +34% missed code detection.
EHR Integration
Production integrations with PointClickCare and Gehrimed. MatrixCare, Netsmart, and other systems via HL7 FHIR, ADT feeds, and custom data exchange. Bidirectional data flow, pulling clinical data for AI and pushing insights back into the clinician's workflow.
Operational Analytics
Cross-facility dashboards for census tracking, quality metrics, staffing optimization, and financial performance. Data infrastructure that turns fragmented systems into a single source of truth.
Every Setting Has Different IT Needs
Post-acute care spans 14+ settings with different regulatory frameworks, payment models, and technology requirements. We build for each one, not a one-size-fits-all platform that fits none of them well.
Skilled Nursing (SNFs)
PDPM reimbursement tied to MDS accuracy. After-hours coverage gaps. PointClickCare/MatrixCare integration.
IT needs: MDS optimization, virtual care, ambient documentation, census management
Home Health (HHAs)
PDGM payment model. Mobile-first workflows. Nurses in rural areas with limited connectivity. OASIS assessments.
IT needs: Offline-capable mobile apps, visit verification, route optimization, remote documentation
Hospice
Medicare Hospice Benefit. Comfort-focused care plans. Family communication across multiple caregivers. IDG coordination.
IT needs: Symptom tracking, family portals, interdisciplinary team coordination, bereavement support
Assisted Living & Memory Care
State-regulated (not Medicare). Medication management. Cognitive decline monitoring. Family engagement expectations.
IT needs: eMAR, behavior tracking, wander management, simplified resident-facing interfaces, family portals
Adult Day Health
Daytime clinical and social programming for medically complex or cognitively impaired individuals. Attendance tracking. Health monitoring during program hours.
IT needs: Attendance management, health monitoring, activity tracking, caregiver communication
CCRCs / Life Plan Communities
Multi-level campuses spanning independent living through skilled care. Residents transition across levels. Different billing at each level.
IT needs: Cross-level care tracking, transition management, unified resident record, multi-payer billing
IRFs & LTACHs
Intensive therapy tracking (IRF). Medically complex patients with 25+ day stays (LTACH). FIM scores. Ventilator weaning protocols.
IT needs: Therapy outcome tracking, complex care coordination, specialized clinical documentation
PACE Programs
Integrated Medicare/Medicaid model for nursing-home-eligible individuals living in the community. Comprehensive care coordination across all services.
IT needs: Integrated care management, dual-eligible billing, transportation coordination, day center operations
Care Transitions
Acute-to-post-acute handoffs. Medication reconciliation. Discharge planning. Readmission prevention across the continuum.
IT needs: ADT alerts, interoperability, care plan continuity, transition tracking, readmission risk scoring
Post-Acute Technology in Production
NeverAlone Virtual Care Platform
24/7 clinical coverage across 130+ skilled nursing facilities in 7 states. EHR-integrated, SBAR-based triage.
Calls Completed
Treat-in-Place
AI-Powered MDS Optimization
AI-driven MDS coding for one of the nation's largest post-acute care providers across 350+ facilities.
PDPM Revenue
Quality Incentives
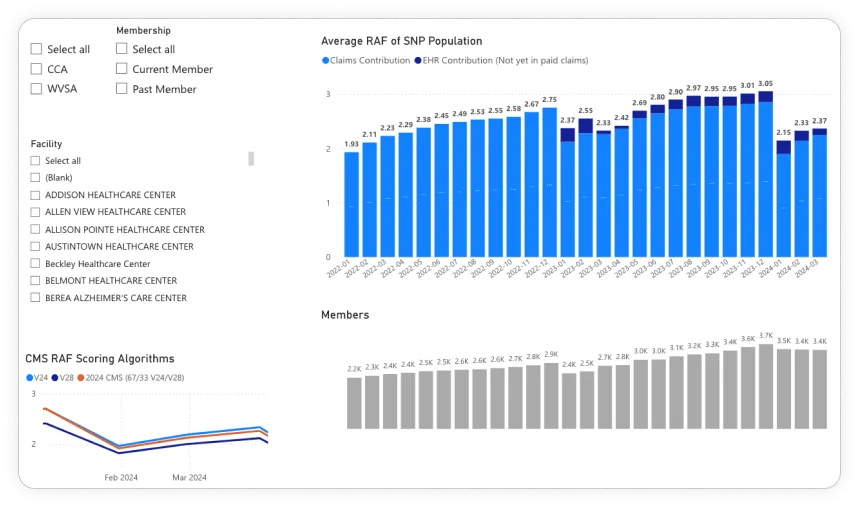
RAF/HCC Code Optimization
AI analyzing EHR and claims data to identify missed diagnosis codes for Medicare Advantage populations.
Revenue Impact
Missed Codes Found
Start Small. Prove Value. Then Scale.
We don't do multi-year contracts or enterprise-wide mandates. We start with a focused pilot, measure real outcomes, and expand only after the data justifies it.
Phase I
Discover
What are the pain points?
Workflow Assessment
Map clinical, operational, & financial workflows
ROI Opportunity
Quantify revenue leakage & cost reduction
Phase II
Experiment
Does it work here?
Pilot Deployment
5-10 facilities, 90 days, clear metrics
Outcome Measurement
Treat-in-place, satisfaction, ROI
Phase III
Engineer
Scale it.
Enterprise Rollout
Expand across your facility network
EHR Integration
Deep integration across all sites
Training & Adoption
Clinical staff onboarding at scale
30-Day Go-Live
Turnkey per facility cohort
Phase IV
Optimize
Make it better.
Performance Tracking
Cross-facility outcomes dashboard
Continuous Improvement
New capabilities, ongoing support (BOT)
We're not learning post-acute care on your dime.
We've built and operated technology in production across 130+ post-acute facilities. We understand PDPM, MDS, SBAR, treat-in-place, and clinical workflows because we live in this space.
Every Project Ships
Industry average is 5%. Every DS project goes to production.
Calendar Year ROI
$10M+ PDPM. $2.4M+ RAF. 45 min → 5 min documentation.
Senior US Team, AI-Accelerated
US-based senior architecture and development, amplified by AI for throughput and quality. Same timezone, HIPAA-compliant.
"NeverAlone has transformed how we deliver care at CommuniCare Health Services, enabling us to provide better patient care and achieve stronger clinical outcomes. By supporting over 130 skilled nursing facilities 24/7, their solution ensures we can meet patients' needs more effectively."
Dr. Matthew Wayne
Chief Medical Officer, CommuniCare Health Services
"I have worked with many technology teams during my career, and Digital Scientists is one of the best. They take the time to understand the customers' needs, deliver innovative solutions, are always professional, and work with your team as a true partner to achieve success."
Amy Severino
Chief Innovation Officer, NeverAlone
"NeverAlone has made our processes more efficient, reducing onsite visits while maintaining high-quality care. It's empowered our individuals to live more independently."
Donna K. Elbrecht
President & CEO, Easterseals Arc of Northeast Indiana
We Work With Your Existing Systems
We don't replace your EHR. We build technology that extends it, integrating with the platforms your clinical teams already use.
EHR Platforms
PointClickCare and Gehrimed in production. MatrixCare and Netsmart via FHIR/HL7/ADT.
Cloud & Infrastructure
AWS, HIPAA-compliant hosting, VPC isolation, real-time processing
AI & Analytics
OpenAI, LangChain, PyTorch, custom NLP, Tableau, Power BI
Let's start with a conversation.
No pitch deck. No demo. Just 30 minutes to share what we've learned building technology for post-acute care and hear what matters to your organization.
Or call: 404.654.3855
HIPAA Compliance & PHI Security
Every system we build is HIPAA-compliant from day one. Encryption, access controls, audit trails, BAA compliance, and PHI de-identification, because post-acute care operators can't afford security as an afterthought.
Learn more about our security approach →
Built With
Healthcare AI Development
Custom AI for clinical documentation, coding optimization, and predictive analytics.
Data Analytics & Engineering
Cross-facility dashboards, data pipelines, and operational analytics.
UX Design & Research
Interfaces designed for busy nurses, MDS coordinators, and clinical staff.
MDS/PDPM Optimization
AI-powered MDS coding for accurate PDPM reimbursement.
Ambient AI Scribes
Documentation automation via HealthContext.AI, 45 min → 5 min.
EHR Integrations
PointClickCare and Gehrimed in production. MatrixCare via FHIR/HL7. Bidirectional data flow.


Common Questions About Post-Acute Technology
What is post-acute care technology?
Post-acute care technology encompasses the digital systems that support patient care after an acute hospital event, across skilled nursing facilities, home health agencies, hospice, assisted living, rehabilitation facilities, and other settings. This includes virtual care platforms, MDS/PDPM optimization tools, ambient documentation AI, EHR integration, clinical decision support, and operational analytics.
How does virtual care work in skilled nursing facilities?
Virtual care in SNFs connects on-site nursing staff with remote clinical providers for real-time consultation, typically during after-hours when physician coverage is limited. The nurse selects a resident, enters SBAR-based clinical information, and connects to a provider in under 3 minutes. Digital Scientists built NeverAlone, which has completed 100,000+ calls across 130+ facilities with a 96% treat-in-place rate.
What is MDS optimization and how does AI improve it?
The MDS is a standardized assessment that determines PDPM reimbursement for skilled nursing. AI-powered MDS optimization cross-references the resident's full clinical record against the MDS to flag diagnoses and therapy minutes that appear in the chart but weren't captured. DS has recovered $10M+ in PDPM revenue and $2M+ in quality incentives for CommuniCare.
How do you integrate with PointClickCare and other EHRs?
We have production integrations with PointClickCare and Gehrimed on platforms we operate. For MatrixCare, Netsmart, and other systems we integrate via HL7 FHIR APIs, ADT feeds, and custom data exchange. We don't replace your EHR, we build alongside it. Our integrations pull patient data for AI analysis and virtual care, then push orders and documentation back into the clinician's workflow. No separate login, no duplicate data entry.
What is the ROI of post-acute care technology?
$20M+ in verified ROI across post-acute clients. $10M+ PDPM recovery, $2.4M+ RAF revenue, $2M+ quality incentives, 96% treat-in-place (avoiding $10K+ per ER transfer), documentation reduced from 45 to 5 minutes, and 95% nurse approval for NeverAlone.
How long does deployment take across multiple facilities?
30 days per facility cohort, including devices, training, credentialing, and EHR integration. We start with a focused pilot of 5-10 facilities, measure outcomes over 90 days, and expand after the data justifies it. NeverAlone was deployed across CommuniCare's 130+ facilities using this approach.
Do you work across the full post-acute continuum?
Yes, SNFs, home health, hospice, assisted living, memory care, CCRCs, IRFs, LTACHs, PACE, adult day health, and transitional care. Each setting has different regulatory frameworks and payment models. Our technology is designed to work across this continuum, recovery, chronic care management, and care transitions from acute events. We also serve IDD services as a related but distinct market.