Agency spend is a planning failure, not a hiring problem.
Healthcare leaders are running multi-facility operations on scheduling tools designed for static workforces. The result is reactive agency calls, overtime that nobody saw coming, and credential gaps that surface in surveys instead of dashboards. Custom workforce intelligence makes the cost visible while the decision is still in your hands.
Agency Spend Cut
Overtime Reduction
Entry-Point Pilot
Analytics Depth
Multi-facility workforce analytics with credential, cost, and capacity views
Scheduling fills shifts. Workforce intelligence answers operating questions.
Healthcare workforce intelligence is the connected system that combines real-time labor cost analytics, credential compliance tracking, predictive scheduling, and operational dashboards across a multi-facility network. It connects HRIS, EHR, scheduling, payroll, and credentialing data into a single view that the COO, CNO, CFO, and VP of HR all need but rarely share.
Buying a scheduling tool is not the same as building workforce intelligence. Scheduling is the easy part. The hard parts are the credential rules engine, the multi-facility cost model, the agency-fill prediction, and the operational discipline to make labor decisions in front of the budget instead of behind it.
The workforce shortage is not getting better. The cost visibility has to.
Healthcare is short roughly 100,000 nurses today and projected to be short 1.1 million by 2030. Operators are running multi-facility, multi-credential, multi-union operations on tools that assume static workforce models. The economics are brutal and the visibility is worse.
Per Resident Per Month SaaS
A 5,000-bed network paying SaaS rates spends $900K annually on workforce tools that flatten operational reality.
Agency Premium
Agency staffing costs three to five times the equivalent permanent rate. Reactive calls compound the problem.
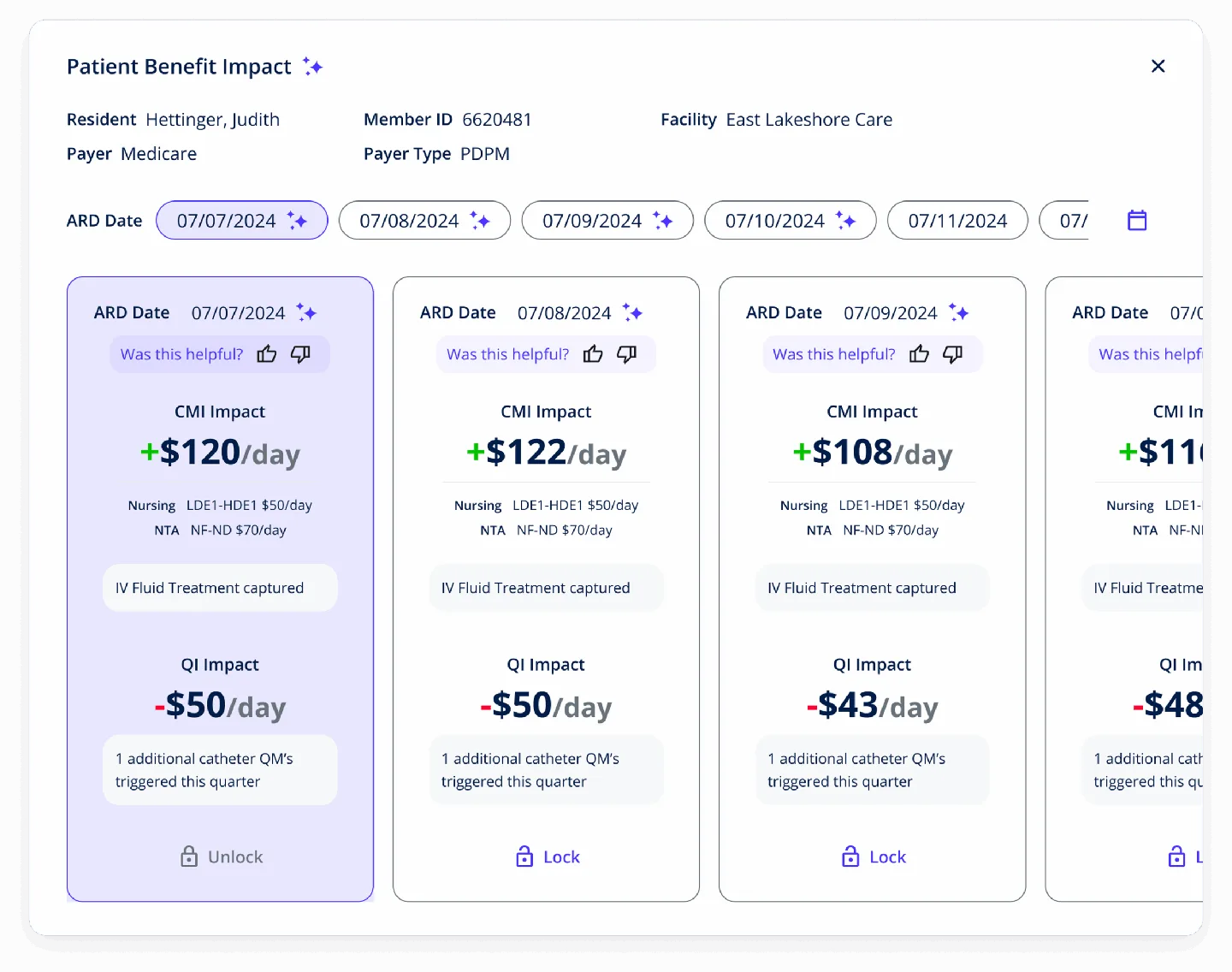
Credential Gaps Surface Late
Most networks discover credential lapses during state surveys, not on a Tuesday dashboard. The cost of finding out late is bigger than the credential.
HR + Clinical Disconnect
Clinical workload data lives in the EHR. Labor cost data lives in HRIS. The questions a COO asks span both.
Workforce intelligence wherever care happens.
Different settings have different staffing rules, credential requirements, and cost structures. The platform model adapts to each. The operational discipline does not.
Skilled Nursing
PPD ratios, credential compliance, agency-fill prediction, MDS-aligned care-hour analysis.
Assisted & Independent Living
Mixed-credential staffing, resident-acuity-aware scheduling, multi-property cost roll-up.
Home Health & Hospice
Visit-based productivity, drive-time cost, OASIS-aligned visit scheduling, contractor management.
Intelligent Scheduling
AI-powered shift prediction, agency-fill probability, credential-aware fill suggestions.
Health Systems & Acute Care
Department-level overtime visibility, float pool optimization, contract-labor analytics.
ACOs & VBC Networks
Labor cost tied to attributable outcomes, care-hour-per-member analytics, productivity benchmarking.
IDD Services
Direct support professional scheduling, multi-residence coordination, behavior-aware staffing.
Behavioral Health & Multi-State Networks
Therapist credential tracking, multi-state licensing logic, telehealth-aware scheduling.
Buy. Build. Partner.
The default workforce stack is a commercial scheduling tool plus a BI dashboard your team built in Tableau. Build is the rare ground-up project. Partner is the lane DS was built for: you drive the operational model and own the IP, we bring data engineering and the operational discipline to make it run.
| Decision Lever | Buy (Smartlinx, OnShift, UKG) | Build (Ground Up) | Partner with DS |
|---|---|---|---|
| Time to working dashboard | Weeks | 12 to 18 months | 8 to 12 weeks for the labor analytics pilot |
| Workforce model fit | Static, generic, configurable to a point | Exact fit, you carry all the risk | Exact fit, configurable rules engine |
| Cost economics at scale | Per-resident or per-employee SaaS | Capex heavy, opex light | Predictable, milestone-funded |
| IP ownership | Vendor owns it | You own it | You own it |
| Multi-facility roll-up | Often per-facility silos | Yours to architect | Multi-facility-aware from the start |
| Best fit for | Single-facility, single-credential operations | Ventures with deep tech teams | Multi-facility post-acute, health systems, home health, hospice, ACOs, IDD networks, behavioral health |
Three layers, one operating view.
Workforce intelligence that operations teams actually use has three layers. Skip any of them and you ship a dashboard nobody opens after the first week.
Data Integration
HRIS, scheduling, payroll, EHR clinical workload, credentialing, and agency-vendor feeds connected into one operational data layer with shared identity and time alignment.
Predictive Scheduling
Shift-gap prediction, agency-call probability, credential-aware fill suggestions, and acuity-driven staffing models tuned to your facility mix.
Operational Dashboards
Role-specific views for the COO, CFO, CNO, VP HR, and unit-level managers. The same underlying data, surfaced in the metrics each role acts on.
Professional Services or Venture Studio.
DS operates two business models. Workforce intelligence engagements typically begin in Professional Services. When the model is differentiated enough to be a product line of its own, the Venture Studio path becomes available.
Build a custom workforce platform for your network.
You operate the network. You own the operational rules. We engineer the data layer, predictive models, and dashboards. Milestone-funded, with a labor analytics pilot as the entry point and phased expansion into predictive scheduling and operational dashboards.
Typical engagement: $150K to $600K. ROI in 12 to 18 months. $100K labor-analytics dashboard as the entry point.
Co-build a workforce platform with equity alignment.
For operators who see workforce intelligence as a competitive moat or a future product, the Venture Studio path aligns incentives via equity or revenue share. We bring the engineering, you bring the operational model, both sides have skin in the game.
Typical engagement: Equity or revenue-share aligned. Multi-year buildout. Skin-in-the-game model designed for operators planning to license the platform externally over time.
Operational analytics at scale. Healthcare workforce models in production.
Workforce intelligence draws on two distinct DS capabilities: large-scale operational data engineering, and healthcare workforce model expertise. We bring proof of both.
24/7 multi-state clinical workforce in production.
We operate the clinical scheduling logic for 26,000+ patients across 7 states. Multi-state provider licensing, on-call rotation, credential-aware shift assignment, and agency-fallback logic running in production every night.
Multi-State
Clinical Coverage
Aware Routing
7-Year Mailchimp BI Partnership
Multi-million-user data platform partnership.
Adjacent capability proof: 7 years building data analytics platforms at multi-million-user scale for Mailchimp (acquired by Intuit). The data engineering, real-time analytics, and dashboard discipline that workforce intelligence requires.
Partnership
Analytics
User Scale
Workforce Intelligence Diagnostic
Before we build anything, we audit your scheduling and HRIS stack, map your agency-spend and overtime patterns by facility, and quantify what custom workforce intelligence can recover.
What You Get
Workforce Cost Map
Agency, overtime, and contract-labor patterns by facility, unit, and credential type
Stack Audit
HRIS, scheduling, payroll, credentialing, and EHR integration gaps
Intervention Inventory
5 to 10 highest-impact intervention points scored by dollar impact and feasibility
Buy / Build / Partner Recommendation
With ROI projections, capital phasing, and CFO-grade business case
60 to 90 Day Pilot Plan
Tied to the highest-impact intervention with a measurable cost outcome
Multi-Facility Rules Brief
Credential, union, agency, and facility-specific rule patterns documented for engineering
HRIS, scheduling, EHR, and credentialing in one operational view
Workforce intelligence that ignores half the data is half a system. We have production experience integrating across the categories your operations team is already running.
HRIS & Payroll
Workday, ADP, Paycom, UKG. Employee record, pay rate, benefit cost, contract type, union status.
Scheduling Platforms
Smartlinx, OnShift, Kronos, ShiftWise. Shift assignments, agency calls, fill patterns, on-call rotations.
EHR Clinical Workload
PointClickCare, Epic, Gehrimed, Netsmart. Clinical activity, patient acuity, care-hour requirements per unit.
Credentialing Systems
License, certification, and competency tracking integrated with state-specific renewal and survey readiness.
EHR Integrations is the supporting capability that runs underneath every healthcare domain at DS. See the production EHR integration backbone →
We do not just build and hand off. We operate, support, and stand behind our work.
Discover
Workforce Cost Map. Agency, overtime, and contract-labor patterns by facility, unit, credential.
Stack Audit. HRIS, scheduling, payroll, EHR integration gaps documented.
Experiment
Hypothesis & Scope. Highest-impact intervention point gets a working dashboard pilot.
Build & Validate. Real labor data, real facility scope, real cost outcome.
Engineer
Iterative Sprints. Operations team feedback loops every 2 weeks.
Systems Integration. HRIS, scheduling, EHR, credentialing connected.
Rules Engine Build. Multi-facility, multi-credential, multi-union rule sets.
Production Deploy. Phased rollout with KPI monitoring.
Optimize
KPI Accountability. Agency spend, overtime, fill rate, validated by analyst.
Continuous Improvement. Model retraining, rules updates, ongoing support.
Patient No-Show Prediction
Reduce no-show rates by 20 to 40% with AI-powered scheduling optimization. Direct workforce-intelligence lever: every prevented no-show is a recovered care hour and a billing event that survives.
See the framework →Often combined with
MDS / PDPM
Care-hour requirements drive PDPM reimbursement. Workforce intelligence connects labor to revenue.
Learn more →Value-Based Care
Labor cost tied to attributable outcomes. Care-hour-per-member analytics, productivity benchmarking.
Learn more →Virtual Care Platforms
Virtual care extends nursing capacity 3x. Workforce intelligence quantifies the operational lift.
Learn more →Healthcare Data Engineering
The capability layer underneath workforce intelligence. Multi-source data integration at scale.
Learn more →EHR Integrations
The supporting capability that runs underneath every domain. Bidirectional FHIR/HL7 in production.
Learn more →Frequently Asked Questions
Common questions about custom healthcare workforce intelligence platform development.
DS works as a Professional Services build partner or as a Venture Studio with equity-aligned partnerships, accelerators, and operator-founder programs. The right model depends on whether you own the IP, share it, or license ours.
See all engagement models →Ready to make agency spend visible while the decision is still in your hands?
Start with a Workforce Intelligence Diagnostic. 2 to 3 weeks. We will map your labor cost patterns, audit your stack, and recommend buy, build, or partner with hard ROI numbers.
Or call: 404.654.3855