Technology built for the reality of post-acute care
Multi-site operators face staffing shortages, reimbursement complexity, and after-hours coverage gaps. We build production-proven technology that solves these problems at scale.

Treat-in-Place Rate
Facilities Deployed
Nurse Approval
To Go-Live
Post-acute care operators are fighting on three fronts simultaneously
After-Hours Coverage
One RN covering 100+ residents at 2am. When something goes wrong, the options are manage alone, call 911, or send to the ER. Each avoidable transfer costs $10K+ and triggers Medicare penalties.
Staffing Shortages
The labor crisis hits hardest on nights and weekends. Nurses are making critical decisions without clinical backup. Burnout drives turnover, which deepens the shortage. The cycle compounds.
Reimbursement Leakage
PDPM ties revenue directly to MDS accuracy. Across 100+ facilities, inconsistent coding leaves millions on the table annually. Manual reviews catch some gaps. AI catches the rest.
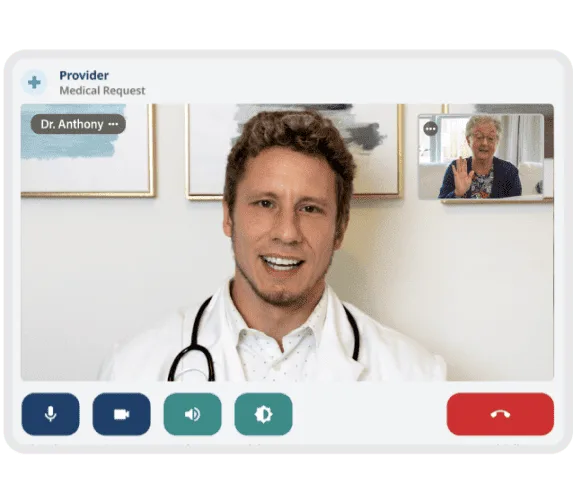
NeverAlone: 24/7 clinical coverage purpose-built for post-acute care
Not generic telemedicine. A workflow-driven clinical platform with EHR integration, SBAR-based triage, and automated care coordination. Deployed enterprise-wide by CommuniCare Health Services across 130+ skilled nursing facilities.
One-touch connection — nurse selects resident, enters SBAR, connected to provider in under 3 minutes
EHR-integrated — patient data, vitals, and medication list pre-loaded into every encounter
Full care coordination — orders, documentation, follow-up, and EMS dispatch when needed
Multi-state credentialing — we handle provider licensing across every state you operate in
30-day deployment — turnkey implementation including devices, training, and credentialing

"NeverAlone transformed how we deliver care — enabling better patient care and stronger clinical outcomes across our 130+ facilities."
Dr. Matthew Wayne
CEO/CMO, CommuniCare Health Services
MDS Section I — Diagnosis
COPD documented in progress notes but not coded on MDS
MDS Section O — Therapies
Respiratory therapy minutes not captured in assessment
MDS Section K — Nutrition
Parenteral/IV feeding documented but weight loss trigger missed
Estimated annual revenue impact: $73,000 per facility
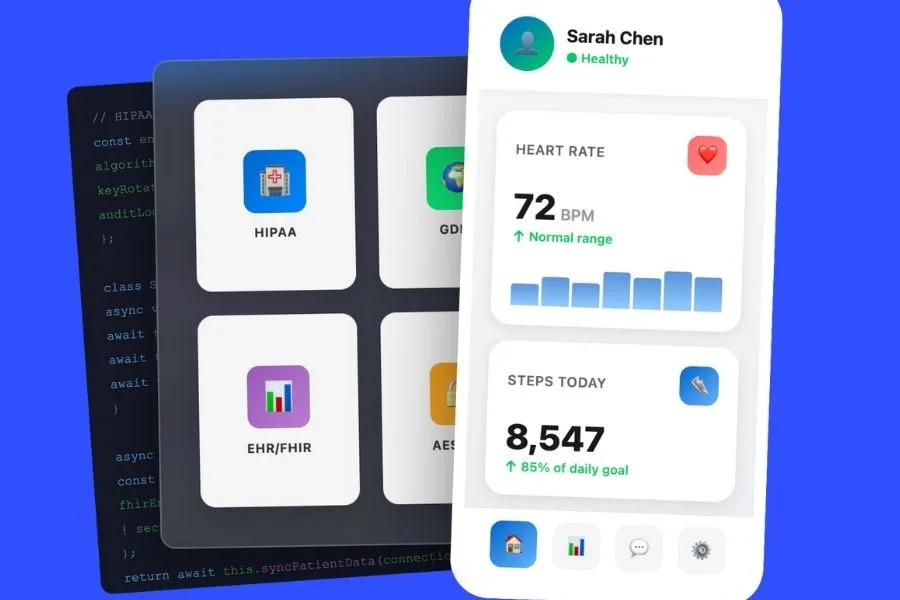
AI-driven MDS auditing that catches what manual reviews miss
Under PDPM, every missed diagnosis, unchecked comorbidity, or incomplete MDS section translates directly to lower reimbursement. Across 100+ facilities, these gaps compound to millions annually.
Our pre-submission audit tool cross-references the resident's full clinical record against the MDS and flags items that appear in the chart but not on the assessment. Not replacing your MDS coordinators — giving them a second set of eyes that never misses a shift.
We're not learning post-acute care on your dime
We've built and operated healthcare technology in production across 130+ facilities. We understand PDPM, MDS, SBAR, treat-in-place, and clinical workflows because we live in this space.
Ship Rate
Every project we build goes to production. Industry average is 5%.
To MVP
Fast iteration with clinical-grade quality and compliance.
Atlanta-Based
Local partner. Not an offshore team or a remote-only agency.
Compliant by Default
Security and compliance built in from day one, not bolted on.
Start small. Prove value. Then scale.
We don't do multi-year contracts or enterprise-wide mandates. We start with a focused pilot, measure real outcomes, and expand only after the data justifies it.
Discovery
2 weeks. We learn your workflows, systems, and priorities before writing a line of code or deploying a device.
Pilot
5-10 facilities. 90 days. Clear success metrics agreed upfront. Turnkey deployment with training and support.
Measure
Treat-in-place rate. Nurse satisfaction. Avoided transfers. Reimbursement impact. Honest results, not cherry-picked metrics.
Scale
Expand across your network only after results justify it. If they don't, we part ways with no hard feelings.
Let's start with a conversation
No pitch deck. No demo. Just 30 minutes to share what we've learned building technology for post-acute care and hear what matters to your organization.
Start a ConversationRelated Insights
From Our Blog

Managing Architecture and Telehealth to Combat the Rise of the Financial Crisis
Dec 12, 2023
Healthcare App Development in 2026: A Guide for Business Leaders
Jan 16, 2026

How Mobile Technology Is Reshaping the Future of Healthcare
Sep 10, 2025